 The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.
The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.It was written in german and was translated into more than 10 languages already. German is not freely available, as the rights are held by a publisher, but all these translations are available as ebooks / PDFs for free, as a gift of Björn for you, for the New Earth, for a new time.
In cooperation with Björn, it is splitted on "Disease is Different" into the sections by organ systems and combined with the real cases of our international testimonial / report archive of the related organ system.
RECTUM AND ANUS
In human beings, the rectum, including the anus, is about 15-30 cm (6-12 in) long. The last four centimeters (1.5 in) are considered the anus. This serves as a temporary storage area for feces.
What is special about this last section of the intestine is that the old intestinal mucosa – from outside the body to about 12 cm into the rectum – is overgrown by ectodermal squamous epithelium.
Thus, we find both superficial ectodermal and sub-endodermal tissue with two differing conflict contents.
External Anal Sphincter
(striated muscle)
Identity conflict
Superficial Rectal and Anal Mucosa (extodermal)
Identity conflict
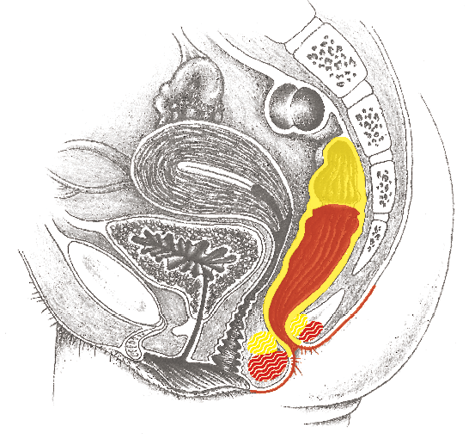
Deep-lying Rectal and Anal Mucosa (endodermal)
Indigestible-anger, not being able to eliminate something
Internal Anal Sphincter
(smooth muscle)
Not being able to hold back/eliminate the feces
Rectal cancer (adeno-ca)
| Conflict | Chunk conflict (see explanations p. 15, 16): indigestible-anger, not being able to get rid of something unpleasant, “crap.” |
|---|---|
| Examples | ➜ Somebody is unjustly accused or put at a terrible disadvantage. ➜ Somebody is betrayed by a friend.  The patient‘s son has taken up with a bad crowd. Together with his friends, he ends up in court. The patient is sure that her son has been caught in a trap and that is why he is being prosecuted = indigestible–anger > growth of a rectal cancer in the active–phase. Half a year later, this is diagnosed by CM. (Archive B. Eybl) The patient‘s son has taken up with a bad crowd. Together with his friends, he ends up in court. The patient is sure that her son has been caught in a trap and that is why he is being prosecuted = indigestible–anger > growth of a rectal cancer in the active–phase. Half a year later, this is diagnosed by CM. (Archive B. Eybl) |
| Conflict-active | Increased function, growth of a cauliflower-like tumor of secretory quality by a conflict aspect of not being able to get rid of something or a flat-growing adeno-ca of absorptive quality, through a conflict aspect of not being able to assimilate something. |
| Bio. function | To better be able to digest or resorb the anger chunk with more intestinal cells. |
| Repair phase | Inflammation of the rectum, possibly also diagnosed as “anorectal abscess“ (see below). Tubercular, caseating, necrotizing degradation of the tumor via acid-resistant fungi and bacteria (mycobacteria), mild fever, night sweats, bright-red blood and mucus in the stool, diarrhea. If bacteria are not present: encapsulation. |
| Therapy | Identify the conflict and conditioning and, if possible, resolve them in real life if still active. Questions: see: p.246. Guiding principle: “I accept the situation and will resolve it with God‘s help.“ Surgery if tumor is too large. Better earlier than later, because today, small tumors are diagnosed as “benign“ by CM. > Less stress for the person concerned. See also remedies for the rectum/hemorrhoids p. 252. |
Hemorrhoids (internal, rare), anorectal abscess1
Same SBS as above.
| Example | A 46-year-old, right-handed woman sweats for the last four nights. On the toilet, she has pain when she presses and when she wipes herself, she finds blood on the toilet paper. Conflict history: five weeks ago, the patient spoke with her mother-in-law on the phone. During the conversation, they talked about dividing up the inheritance they received from the recently deceased grandmother. (The patient is legally no heiress, but her husband is.) On the phone, the mother-in-law said to her, “Anyway, it only concerns the children.“ With this, the patient assumed that she is not invited to this meeting. On the day before the first symptoms appeared, her mother-in-law comes to visit and is very kind to her = conflict resolution > bleeding removal of the tumor in the following days = repair phase. (Archive B. Eybl) |
|---|---|
| Phase | Repair phase: A small tumor usually develops unnoticed under the epithelium layer during the conflict-active phase. It is not noticed until the repair phase, when it breaks open = CM: “hemorrhoids,“ “rectal abscess“ > night sweats, mild fever, pus, bright-red blood. Usually a recurring–conflict. |
| Note | The most important difference between this and the more common, superficial hemorrhoids is the fever and night sweats in the repair phase. |
| Therapy | The conflict is resolved. Support the healing. If recurring, find out the conflict and conditioning and resolve them. Questions: see: p.246. See also remedies for the rectum/hemorrhoids p. 252. |
1 See Dr. Hamer, Charts p. 28
Hemorrhoids (superficial, common)1
| Conflict | Identity conflict – not knowing where one belongs, not knowing which decision to make, not knowing which partner to choose. Often, the conflict has something to do with the mother (mother = identity). Less often, territorial-anger conflict. |
|---|---|
| Examples | ➜ A child doesn’t know where it belongs after its parents get divorced. ➜ Doubts as to whether a move/career change was the right decision. A seven-year-old boy loses his father. After that, his mother has various partners, who treat the boy very badly; they even abuse him = identity conflict. (See Dr. Hamer, Goldenes Buch Bd. 2, p. 397) A 69-year-old patient lets himself undergo chemotherapy for cancer of the prostate gland. However, he becomes doubtful as to whether he is doing the right thing. “Should I continue the treatment?“ = identity conflict. (See Dr. Hamer, Celler Dokumentation, p. 61) A married women falls in love with another man. She doesn‘t know whether she should divorce her husband for the sake of the other man = identity conflict. Cell degradation in the anal epithelium. Restoration with bleeding in the repair phase. (Archive B. Eybl) |
| Conflict-active | Reduced sensibility of the anal mucosa, simultaneous slackening of the anal sphincter muscles. Later, degradation of epithelium = ulcer; tearing of the anal epithelium (anal fissures) are possible > no pain, no bleeding, numbness. One seeks belonging, wrangles with decisions. |
| Bio. function | Widening of the anus to insure better removal of feces. In nature, feces and urine serve to mark territory. The place of defecation defines one‘s living space and the location of the individual. With additional feces, the location can be defined better and the identity is emphasized. Feces-marking takes urine-marking to the next level. |
| Repair phase | Restoration of the degraded substance, pain, swelling, bright-red blood = “hemorrhoids,“ aggravated by syndrome. Usually a recurring–conflict. |
| Repair crisis | Heavy bleeding, possibly chills; if the voluntary anus muscle is also affected, rectal cramps (see below for 2nd possibility) and painful rectal tenesmus (feeling of having to defecate when one doesn’t). |
| Questions | Irritation, bleeding since when? (When it bleeds, the conflict must have been resolved). First time bleeding? (No > also examine the first episodes. Yes > only examine this episode). Which problem did I solve the day before or on the same day? (Good conversation, personal decision, good news, the weekend, vacation)? When this is determined, one automatically knows the conflict. Has the conflict always dealt with certain people or is it about an inner dilemma, having nothing to do with people? (Specify the conflict). What are my earliest experiences with regard to this? (Childhood)? Were my parents also involved in the issue? (> Also, examine the issue in the family and heal through conversation/meditation/forgiveness/prayer). What has conditioned me additionally? Which beliefs nourish this conflict? Am I ready to make a new start? |
| Therapy | Identify the conflict and conditioning and, if possible, resolve them in real life if still active. Guiding principle: “I will make a definite decision. Then, I will know where I belong.“ See also remedies for the rectum/hemorrhoids p. 252. OP if necessary. |
Fissures of the anal epithelium (anal fissures)
Same SBS as above.
| Phase | Conflict-active phase, pain later in the repair phase when the fissures are healing. |
|---|---|
| Therapy | Identify the conflict and conditioning and, if possible, resolve them in real life if still active. See also remedies for the rectum/hemorrhoids p. 252. |
1 See Dr. Hamer, Charts p. 129
Rectal cramps (sphincter spasms, tenesmus)
| Conflict | Chunk conflict (see explanations p. 15, 16), not being able to sufficiently retain the feces. In the figurative sense: One is trying desperately no to bother anyone/not to be intrusive. One always shows great reserve. One would rather sacrifice their territory than become unliked. |
|---|---|
| Example | A woman is in the hospital for a hemorrhoid surgery. She is given an enema to cleanse the colon, and she becomes terribly nauseated. At the last second, she runs to the washbasin where she vomits and at the same time loses control of her bowels: she stands in a puddle of water and excrement. At that very moment, the doctor comes in and tells her to lie down in bed immediately because they want to give her an infusion. Fully soiled, she must lay herself in bed = conflict of not being able to hold back the feces. Since then, the patient suffers from intense rectal spasms. Sixteen years later, at a lecture by Helmut Pilhar, she goes behind the curtain and can resolve the conflict by means of meditation. (See www.germanische-heilkunde.at/index.php/erfahrungsberichte) |
| Conflict-active | Increased muscle tension (hypertony), problems with bowel movement. When the stool is hard, it can only be pressed out with extreme effort, because the inner sphincter does not open completely. |
| Bio. function | Increased tension so that the feces can be held back. Harder feces stink less. |
| Repair phase | Normalization of the muscle tension; in the repair phase crisis: attacks of painful anal cramps. |
| Questions | Was there a real situation where I was not allowed to defecate? Was there a time when I experienced stress during defecation? Am I always reserved? (If yes: to remain well-liked)? Did the mother have to hold her child back during the birth? What are the parents like with regard to letting things out? What still conditions me? (Experiences during childhood). |
| Therapy | Determine the conflict and conditioning and, if possible, resolve them in real life. Transdermal magnesium. |
Compulsive retention of feces by children
| Conflict | Something must not see the light of day, not come out, must be held back because it is ugly or embarrassing. As almost always with children, a substitution conflict (for parents, ancestors). Or the mother’s conflict during birth/pregnancy: “I must hold the child back, so that it doesn’t come out now.” |
|---|---|
| Example | a A 3-year-old girl often suppressed defecation for days, as if defecating was something terrible. The parents tried everything they could think of (poo-poo games, etc.) to no avail. When asked if there is something in the family that shouldn’t come to light, the mother explained that her partner (the father of the child) suffers from a disease that compels him to swear wildly (Tourette syndrome). Understanding this is threatening their marriage, her partner “stifles” these outbursts under great strain. > The child was shouldering her father’s restraint. As the connections became clear and the father’s condition improved, the little one was able to go to the toilet without any trouble. (Archive B. Eybl) |
| Phase | Conflict activity of the internal anal sphincter muscle > persistent tension. |
| Questions | Symptoms since when? What is the child shouldering? (For parents, less often for other ancestors) What family issue isn’t allowed out? What needs to be suppressed/retained? (Taboo issues, something someone is ashamed of, something ugly) |
| Therapy | Determine and resolve the conflict, causal conditioning and belief structures. Transdermal magnesium. |
Encopresis (paradoxical diarrhea) – voluntary or involuntary fecal soiling
By the age of three, children should be toilet trained. If not, the following conflict may come into question:
| Conflict | According to Frauenkron-Hoffmann: The child feels neglected and draws attention to itself through the “scent.” It is basically a call for the mother to take care of the child. According to Dr. Sabbah: The child “senses” a poisoning in ancestors (“the poison must be expelled”). |
|---|---|
| Phase | Conflict activity of the inner sphincter muscle > constant tension. |
| Questions | When did the symptoms begin? (Stress at school/family, divorce, fight, disharmony)? Does the child feel neglected? Was/is there a poisoning among ancestors or parents? (Also consider drugs/medications). |
| Therapy | Determine and resolve the conflict, causal conditioning and beliefs (of the family). |
Diarrhea
Possible causes
- Poisoning: Spoiled or contaminated food, side effect of medication, especially antibiotics and psychopharmaceuticals as well as poisoning with the artificial sweetener, aspartame, etc.
Diarrhea function = elimination of toxin.
- Incorrect diet: Ingesting the wrong combination of foods can promote diarrhea (e.g.: fruit – sugar – grain).
- General sympatheticotonia and anticipatory anxiety: = stress diarrhea (CM: diarrhea-dominant irritable bowel). This affects approximately one in five people worldwide. In anticipation of stress (= sympatheticotonia), the involuntary sphincter muscles of the body open: anal and bladder sphincter for “ballast-shedding,“ gastric sphincter for a speedy passage, pupillary sphincter for easier viewing, etc.
Gaunt, thin, emaciated people are predominantly sympathicotonic, i.e., they are predominantly under stress.
Peace and serenity are missing, little fat can accumulate = athletic or leptosomic people according to Kretschmer. These individuals tend to be “crapping their pants“ at every opportunity. > Loose stools, diarrhea.
A 16-year-old student is an amateur ski racer. On the day of the competition, specifically immediately before the start, he must go to the toilet constantly due to the diarrhea. = General sympatheticotonia, anticipatory anxiety. Later in life, he suffers from diarrhea before important appointments as well. (Archive B. Eybl).
The opposite is the comfortable endomorph (vagotonic), who is a good eater with tendency toward constipation.
- Intestinal muscles: If an indigestible-anger chunk gets lodged in the intestines, two SBSs are usually triggered: An SBS of secretory quality (cauliflower-like tumor), so as to dissolve the chunk with gastric juices and one of motor quality (peristalsis), so as to expel it (conflict of not being able to dislodge something or move it forward).
Diarrhea in the repair phase crisis during the repair phase or in persistent repair, e.g., Crohn‘s disease, colitis, ulcerative colitis. (See: p.243.)
- Liver – gallbladder: Recurring territorial-anger conflict. This type of diarrhea accompanies fat intolerance.
Endodermal liver parenchyma or the ectodermal gallbladder ducts can be affected. Due to a shortage of bile, fat cannot be digested > pulpy, fatty stools that float in the toilet.
Territorial-anger or identity conflict – starvation or existence conflict. (See: p.265)
- Pancreas (rarer): Recurring-conflict. After many bouts of pancreatitis, the glands that produce pancreatic juices deteriorate. Enzymes for the digestion of proteins, fats and starches are then lacking > pulpy, bright, malodorous stools that float. Conflict: trouble with family members, the battle for the chunk, inheritance conflicts. (See: p.274.)
- Thyroid (rarer): the thyroid hormone thyroxin makes the body sympathicotonic. It increases metabolism and promotes the emptying of the bowels. Diarrhea in the conflict-active phase.
Conflict: not being able to grasp or get rid of something, because one is too slow. (See: p.145).
Therapy for diarrhea
Depending on the cause:
- Centering exercises such as tai chi or strength training.
- Foods: blueberries, barley, oats, honey.
- Tea: elecampane, blackberry (dried fruits leaves), oak bark, chamomile, bistort, plantain.
- Zeolite powder internally.
- Possibly Tannalbin tablets.
Bloating, flatulence
Every digestive process results in the production of intestinal gas. However, most of it diffuses into the circulatory system and is expelled through the lungs.
Flatulence denotes an excess of intestinal gas exceeding 0.5 to 1.5 liters per day.
Possible causes
- Improper nutrition: A high percentage of high-fiber foods or an unfavorable combination of foods (e.g., fruit – sugar – grain) can promote flatulence. Legumes (with the sugar molecules rhamnose and stachyose) cause a definite rise in gas production.
- Poisoning due to antibiotics and other chemo-therapeutics: damage of the intestinal flora > incomplete digestion > fermentation > flatulence.
- General sympathicotonia: Gas in combination with diarrhea: signs of a general sympathicotonia (see: p.13). The passage of food is accelerated > incomplete digestion, incomplete air resorption.
- Impaired functioning of the small intestine or colon: Not enough air-resorption due to degeneration of the intestinal mucosa (low resorption capacity). According to Dr. Hamer, intestinal gases help to expand the intestine so that a lodged chunk can be moved onward. Histamine or lactose intolerance can cause strong flatulence, sometimes together with diarrhea. = Indigestible-anger (see pp 239).
- Pancreas or liver: Too little pancreatic juices or bile > incomplete digestion > fermentation > flatulence = anger conflict with family members, the battle for the chunk, inheritance or starvation-existence and territorial-anger or identity conflict respectively.
Three hypotheses
• People who feel they are not being adequately noticed/recognized. Biological meaning: Expression of one’s own presence with an odor mark. I.e., a preliminary stage of feces marking.
• People who keep “inflating” old problems without thinking of solutions. (Ideally, the digestion only deals with only one morsel at a time for a while). Biological meaning: Nature reminds the individual that “inflating” the past only results in a bloated belly and “bad air.”
- If someone says too many unimportant things instead of meaningful things, the body reflects this by producing excessive “air.”
Therapy for flatulence
Depending on the cause (e.g., diet change).
- Movement/gymnastics.
- Deep breathing, so that the gases can be released.
- Hot, full baths, possibly with whole salt or magnesium chloride.
- Tea: anise, fennel, melissa, parsley, linden blossoms.
- Hildegard of Bingen: bay leaf cookie powder special recipe.
- Build-up of symbionts with OMNi-BiOTiC®.
- Symbioflor 2, EM.
- Swallow 1 tsp. whole mustard seeds with water regiment..
- Zeolite powder internally.
Constipation
Possible causes
- Poisoning with medication: Misuse of laxatives, sleeping pills, tranquilizers, antacids, iron preparations, diuretics, blood pressure medication, anti-Parkinson‘s disease medication, antiepileptic drugs, medications for bladder incontinence and morphine (paralyzes the colon due to a permanent contraction of the longitudinal muscles in the intestines).
- Diets that are low in fiber, low in vital substances (cheap, industrial foods).
- Active kidney collecting tubules: Water is collected for when one is on the run (i.e., on a trip) or feels abandoned, so that a shortage of fluids can be survived. The colon thoroughly removes water from the food pulp or feces > hard stool, tendency to constipation. = Refugee and abandonment conflict (see p. 277)
- Too little exercise: A well-functioning intestinal peristaltic is dependent on sufficient exercise. This is not just based on the mechanism of the colon itself; rather, it is linked to the 11th brain nerve (nervus accessorius). Lack of exercise > neglected breathing > under-functioning of the diaphragm (as a muscle aiding digestion).
- General vagotonia: During general parasympatheticotonia, it is common for all of the sphincter muscles of the body, including that of the anus, to be closed tight (see: p.13). Feces is only reluctantly released. People who are primarily vagotonic tend to be constipated. These corpulent, rotund, comfortable endomorphs (according to Kretschmer) are excellent eaters. Food (like life) is enjoyed and digested at leisure. Therapy: look for challenges.
- Intestinal musculature: Constipation in the conflict-active stage (see: p.243):
1. Nothing can help (moving forward) (stagnation).
2. Something is not yet finished, something takes forever and is waiting to be finished.
3. The fear of leaving the old (e.g., traditions, values, home) behind.
Often in combination with indigestible-anger.
- Thyroid: persistent repair, condition following persistent repair. Too little of the thyroid hormone thyroxin results in a lack of drive and slow metabolism > sluggish colon = conflict of not being able to grasp or expel something because of being too slow. (See: p.147.)
- Parathyroid gland: Conflict–active phase of a persistent conflict. An overly high parathyroid hormone level can cause constipation. (See: p.149.)
- Ileus (blockage) by a tumor or twisted intestine (volvulus). Conflict–active phase or repair phase. Acute constipation, possibly with pain, vomiting of feces = indigestible-anger conflict (see p. 245).
1. Nothing can help (moving forward) (stagnation).
2. Something is not yet finished, something takes forever and is waiting to be finished.
3. The fear of leaving the old (e.g., traditions, values, home) behind.
Often in combination with indigestible-anger.
Therapy for constipation
Depending on the cause:
- Physical exercise/sport in order to stimulate the colon. Especially effective: endurance running and after that, gymnastics.
- Making a sharp distinction between resting and active-phases, so that both sympathicus and vagus come to fruition. For example, first exercise and then be really lazy.
- Squatting position while using the toilet: When you squat, the sphincter muscles relax and the rectum comes into a straight position > Feces can be deposited without effort and pressing. > Get a toilet footstool.
- Regular massage of the trapezius and sternocleidomastoid muscle. These two muscles are innervated by the 11th brain nerve and correspond directly to the intestinal muscles.
- In the morning, drink lots of pure water.
- Foods: raw fruits and vegetables, flaxseed, dried fruits, figs, apples, garlic, onions, raw sauerkraut, raw red beets, lettuce.
- Breathing exercises.
- Tea: agrimony, centaury, vermouth, absinthe, common polypody, St. John‘s wort.
- Improve the intestinal flora: Symbioflor 2, EM (see p. 66).
- Enemas/colon cleansing therapy for purging and colon reboot. Such treatments should not activate/trigger conflict, otherwise, don‘t do them! Be cautious, especially with children (invasion of privacy can cause conflicts).
Remedies for the colon
- For acute inflammation: colloidal silver, MMS (see p. 68).
- Do not take unnecessary medications.
- Tea: centaury, agrimony, fennel, peppermint, yarrow, and others.
- Chew food thoroughly – enjoy your food!
- For symbionts: EM (p. 66, Symbioflor 2, kombucha, yogurt.
- Cayce: Eat an almond every day, colon cleansing (water colon cleansing), and enemas for detoxification.
- Hildegard of Bingen: Season with fennel seeds, peppermint. Gentian-powder wine special recipe, absinthe elixir special recipe, sanicle (Sanicula europaea) powder- or elixir special recipe.
- Castor oil compress treatments.
- Warm abdominal compresses with salt water.
- Fasting – the oldest therapy for digestive disturbances. When fasting, we should follow our instincts and feelings, like when animals refuse to eat. Fasting under pressure or coercion triggers new conflicts and new illnesses.
- Willfort: Three-week health cure of drinking 0.5-1 l (16-32 oz) of freshly–squeezed white cabbage juice, distributed throughout the day.
- Zeolite powder, natural borax, internally.
- Treatment: Swallow mustard seed without chewing + medicinal clay + water. Linseed oil.
- Squatting position on the toilet: When squatting, the sphincter muscles relax and the rectum assumes a straightened position > Feces can be released without effort and pressing. > Use a footstool to elevate feet/legs.
All experience reports on the organ system “Rectum – Anus” from the International Report Archive:
| Author | Title and Overview | Keywords | ||||
|---|---|---|---|---|---|---|
 | 2025/03/12   After spontaneous, unannounced exclusion (end of January) from several 5BN Telegram groups because of my business model - development of a hemorrhoid (right) after balancing measures, which then healed (end of February). | Hemorrhoids | ||||
 | 2024/05/08 One evening I had a somewhat heated argument with my husband (it was about correcting his behavior in the presence of other people, my identity and self-determination). And lo and behold: the next morning I woke up and felt a sizeable hemorrhoid on my bottom ... | |||||
| 2024/03/31 The tax office sent me a notification about a letter delivered to the service portal. On Friday evening, of course. However, the service portal was no longer accessible to me, as I am no longer self-employed. So, I couldn’t access the letter. Over the weekend, I became increasingly anxious and worried... | |||||
| 2023/08/13 | |||||
 | 2015/01/01 Here is a list of other sources where experience reports with the 5BN can be found, e.g. to:: Bursitis, conjunctivitis, rheumatism, diabetes, hay fever, psoriasis, bedwetting, stuttering, oceans, aggressive constellation, endometrial CA, cervical cancer, shingles, tinnitus, toothache, heart attack, high blood pressure, colic, slipped disc, knee pain, leukemia, bone cancer, voice gone, stomach pain, hives, Epilepsy, intolerances, Crohn's disease, skin rash, facial paralysis, hiccups, anorexia, bronchitis, corneal inflammation, migraine, thyroid cyst, aphthae, osteolysis, gastritis, rectal spasms, milk duct carcinoma, allergies, hepatic coma, gray hair, nail fungus, heartburn, nasal polyps, caries, heart attack, ankylosing spondylitis, melanoma, psoriasis, water belly, hailstones, prostate, . .. |